
WHAT IS TRIGEMINAL NEURALGIA?
The official description of Trigeminal Neuralgia (TN) is: “sudden, severe, brief, stabbing pain occurring in attacks lasting at the most a few seconds usually only on one side of the face and provoked by light touch”. It is “the worst pain known to man” and attacks are often described by patients as being like ‘an electric shock’, which may be severe enough to rivet them to the spot or bring them to their knees. The pain can also be described as stabbing, shooting, burning, excruciating, and unlike any other pain previously experienced.
The pain attacks may last for a few seconds or occur in “volleys” — multiple bursts of pain in quick succession — lasting several minutes. The pain, often triggered by just a light touch to an area of skin, can strike at any time and without warning. Frequency of attacks can vary from a few times a month to several times each day depending on the severity of the condition. Unfortunately, for most sufferers, the condition is progressive and will worsen over time. Although to date there is no guaranteed cure for the condition, there are several treatments which can give relief.
This is a hidden disability your donations may help us find a cure.

WHERE IS
THE PAIN FELT?
The pain is most felt on one side of the face (unilateral) and usually in the cheek or lower jaw. There may also be pain inside the mouth and often it can feel as if it is coming from one or more teeth, hence many people seek the help of their dentist initially and some may undergo unnecessary dental treatment before getting a correct diagnosis. In other instances, pain can be felt on the entire side of the face or, occasionally, just around the eye and forehead. TN tends to affect the right side of the face more than the left side. Very rarely, it can occur on both sides (this is known as bilateral) but it is rare to have acute pain on both sides at the same time.
WHAT ARE THE CAUSES OF
TRIGEMINAL NEURALGIA?
Although there is still much debate among neuroscientists regarding the causes of TN, it is now generally agreed that the trigeminal nerve is ‘misfiring’ and is sending out inappropriate pain signals. The trigeminal nerve can be thought of as being like an electric wire or cable that contains numerous fibres conveying different messages to the brain. There are pain, touch, temperature, and vibration fibres, each insulated from one another by a protective sheath called myelin. The myelin sheath can be damaged by pressure from blood vessels (veins or arteries), multiple sclerosis (MS), injury to the nerve or simply as part of the ageing process. In a small number of cases, the cause may be due to a tumour or a benign growth pressing on the nerve.
When the nerve is injured, it becomes ‘hyper-excited’. The result is that the nerve fibres inside the nerve itself fire off signals of pain at the least provocation. Pain fibres can “short circuit” with touch fibres, due to loss of insulating myelin, and this results in a “sparking” between the two, sending incorrect pain signals to the brain. The myelin tries to heal itself and this sometimes results in successive periods of remission when no pain occurs.
MORE ABOUT THE
TRIGEMINAL NERVE
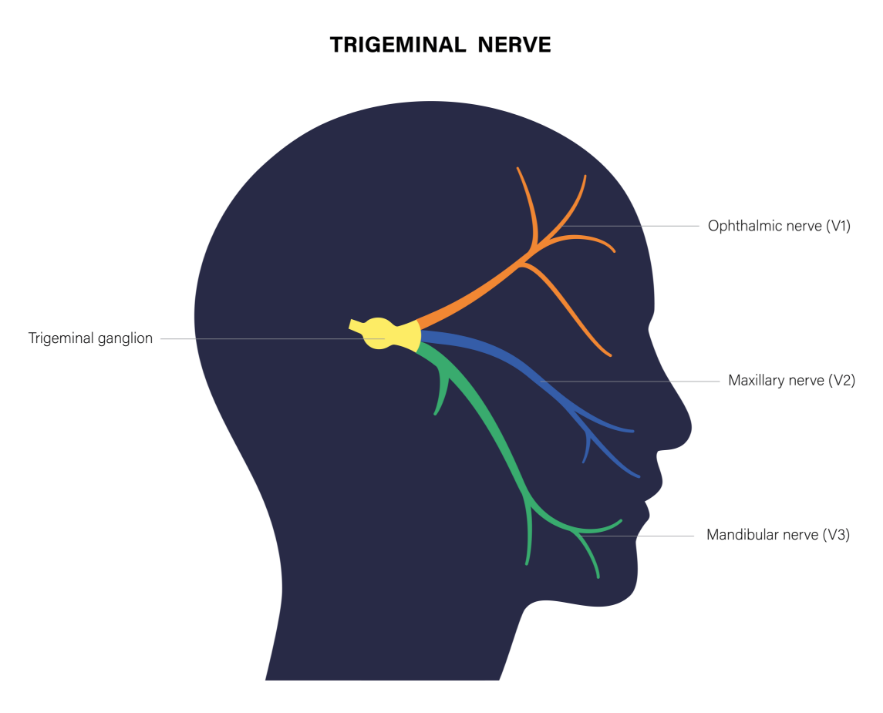
There are 12 pairs of nerves called the cranial nerves which provide the nerve supply to the right and left sides of the head and neck. The trigeminal nerve is the fifth and largest of these and is known medically as ‘V’ since V is the Roman numeral for five. Its job is to provide nerve sensation from the mouth, face and the front of the scalp, as well as controlling the muscles which are used in chewing (mastication). The trigeminal nerve allows us to experience touch, temperature, and pain in the face. It does not affect the way the face looks; that is a different cranial nerve.
There are numerous small nerve fibres in the face which pick up sensations and transmit them to the brain. These fibres progressively gather into three main branches on either side of the face. These are referred to as V1, V2, and V3:
• The ophthalmic branch (V1) which runs through the eye, forehead, and nose
• The mandibular branch (V3) which runs through the lower teeth, gums, and lip
• The Maxillary Branch (V2) Which Runs Through The Upper Teeth, Gums, Lips, Cheek, Lower Eyelid, And Side Of The Nose
PREPARING
FOR CONSULTATION
Your consultation with the neurologist or pain specialist is time-limited and so it is important that you attend with all the necessary information to make the most of the session.
At TNA, we suggest the following:
Complete a pain diary: Binging a pain diary with you is very helpful, it will aid the clinician in diagnosis and monitoring the effects or TN/medications.
• The pain diary should be as detailed as possible.
• It should not be overly long, e.g. perhaps the last 1-2 weeks.
• You should note the times of attacks e.g. 7am, 12pm.
• You should note what you were doing when the attack occurred e.g. brushing your teeth.
• You should describe the pain, e.g. shooting, aching, throbbing, burning.
• You should note how long the pain lasted e.g. was it fleeting? Did it linger?
Write down your questions: This is your chance to ask the specialist what you want and need to know. Write down the questions you need answers to beforehand. Often, appointments go so quickly we may forget or not have an opportunity to get the info we wanted without having these written down.
Tried treatments/medications: If you have already had medicines or treatments, note down what you have had done, how long you tried said treatment for, and if it made any difference (be that for good or worse).
• E.g. Nightguard made by dentist
• E.g. GP prescribed carbamazepine, I took this for 2 weeks.




