
TREATING TN WITH SURGERY
QUICK FACTS
- Surgery is an option when medication is not working or when drug side effects become intolerable.
- The options for surgery should be discussed with a neurosurgeon. Decisions will be based on the age and health, the type of pain, the location of the pain and the patient’s personal quality of life.
- The best procedure is the one with the smallest risk for the patient, while providing the best pain relief with minimal side effects.
- You need not suffer for years before considering surgery; indeed it may be more effective sooner rather than later.
- The vast majority of people with TN do ultimately find relief for their pain.
|
Procedure |
Initial Pain Relief |
* Pain Free at 5 Years |
* Pain Free at 10 Years |
|---|---|---|---|
|
MVD |
93% |
75% |
70% |
|
Radiofrequency Lesioning |
96% |
50% |
40% |
|
Glycerol Injection |
91% |
46% |
N/A |
|
Balloon Compression |
92% |
69% |
62% |
|
Stereotactic Radiosurgery |
67% |
58% |
N/A |
* These are only estimates and variation can be large.
We recommend thoroughly researching all the various options and deciding on the most

MICROVASCULAR DECOMPRESSION (MVD)

PERCUTANEOUS PROCEDURES
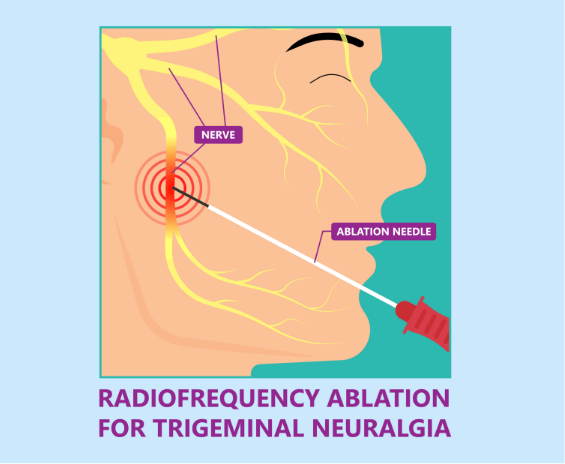
RADIOFREQUENCY LESIONING
GLYCEROL INJECTION

BALLOON COMPRESSION

STEREOTACTIC RADIOSURGERY

YOUR QUESTIONS
WHICH SURGEON SHOULD I USE?
Do not be afraid to question the neurosurgeon! You can request a brain scan to rule out other conditions and perhaps see the cause of the pain. The more experienced the neurosurgeon, the fewer the complications; for MVDs, the surgeon needs to be doing 4-5 procedures a year. But it is important to note that a recurrence of TN is possible after surgery.
I DON’T HAVE ‘TYPICAL’ TN – WILL SURGERY WORK FOR ME?
This depends on a range of factors (see ‘Quick Facts’). In ‘atypical’ cases the full range of procedures is available, but results are not as good. For those with Multiple Sclerosis (MS), through-the-cheek methods are preferred. With Post Herpetic Neuralgia (PHN), medicines, rather than surgery, are most commonly used. Nerve injury pain is also mainly treated with medicines, TENS units or motor-cortex stimulation could be used.
WILL SURGERY STOP MY PAIN?
Whilst the aim of all procedures is to stop or minimise TN symptoms, the recurrence and success rates differ depending on which procedure is used. MVDs may fail for a variety of technical reasons and in some cases, nerve compression may just not be the cause. With radiofrequency lesioning, the surgeon may apply less heat to disrupt the pain transmission, while minimising loss of sensation (numbness). With glycerol injections, the glycerol may drain out of the area where it’s needed, before it has a chance to work. In radiosurgery, even slightly inaccurate targeting can miss the nerve and therefore deliver too little radiation to damage the nerve. Pain relief can also often be delayed.
HOW CAN I FIND OUT MORE?
You may find it useful to talk to other patients who have had surgery. We can put you in touch with others who have undergone various procedures and TNA UK members can contact us for further details about surgeons, specific surgeries or any of the issues covered above.