 Toothache or trigeminal neuralgia? The signs patients and dentists should know
Toothache or trigeminal neuralgia? The signs patients and dentists should know
Why severe facial pain can be mistaken for dental pain
Short answer
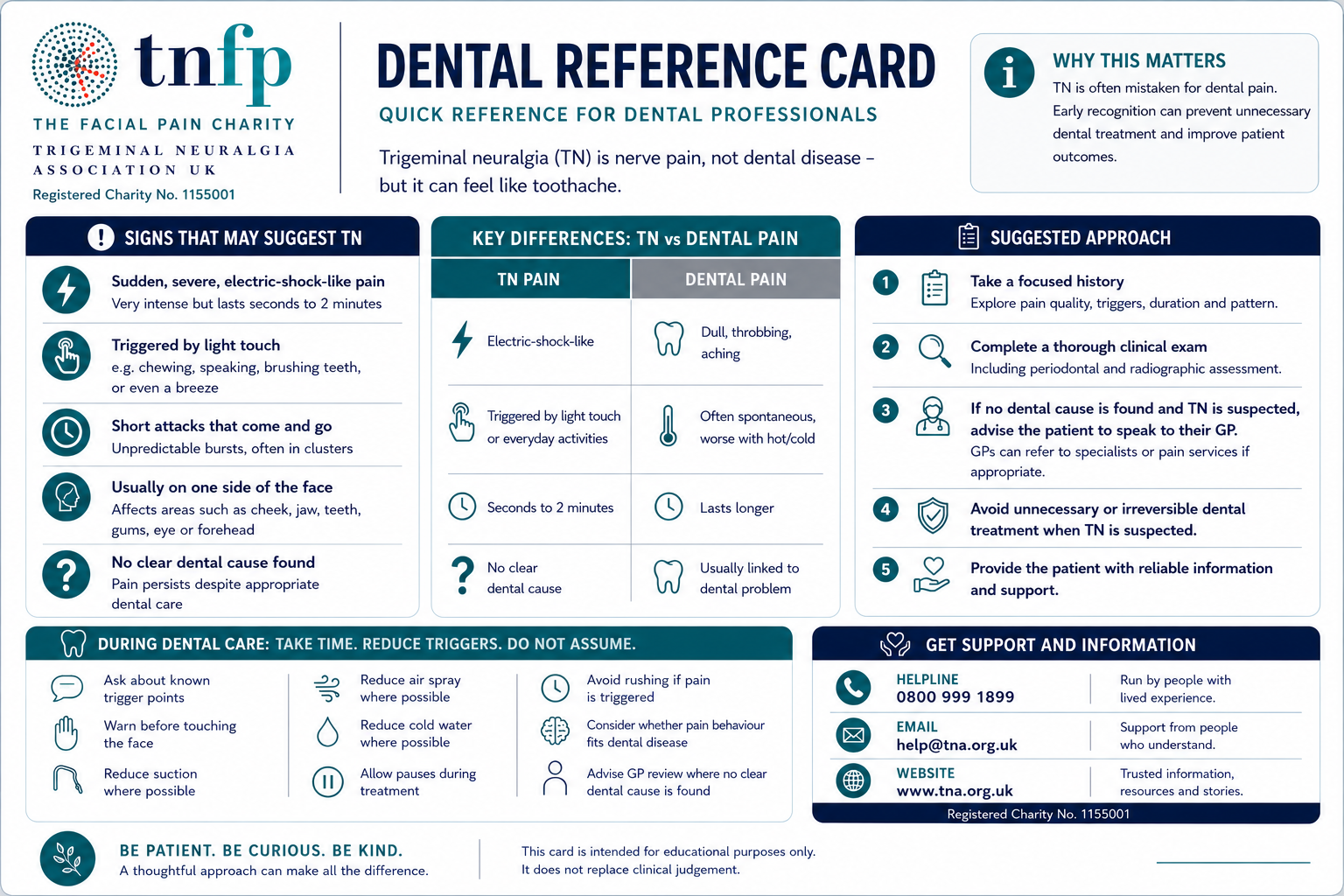
Toothache and trigeminal neuralgia can feel similar because trigeminal neuralgia can cause severe pain in the jaw, teeth or gums. However, trigeminal neuralgia is nerve pain, not dental disease. NHS information describes it as sudden, severe facial pain, often like an electric shock in the jaw, teeth or gums. Therefore, many people see a dentist before they see a GP or specialist.
Dental disease needs dental care. Trigeminal neuralgia needs medical assessment, appropriate treatment and, in some cases, specialist referral. When the cause is unclear, patients should not be left going round in circles.
Not every toothache is trigeminal neuralgia
Not every toothache is trigeminal neuralgia. Dental pain is common and should always be checked properly by a dentist.
The concern comes when severe, electric-shock-like facial pain continues, and dental causes are not found. That is where the gap opens. The pain may sound dental, but behaves like nerve pain.
This article is not a diagnosis tool. It is a guide to the signs that patients, dentists and GPs should notice when facial pain does not follow a typical dental pattern.
Why trigeminal neuralgia can feel like a toothache
The trigeminal nerve carries sensation from the face, teeth, gums and jaw to the brain. When trigeminal neuralgia affects that nerve, the pain can feel as if it comes from a tooth, even when the tooth is healthy.
The NHS says trigeminal neuralgia pain can affect the teeth, lower jaw, upper jaw or cheek. Less commonly, it can also affect the forehead or eye. The pain usually comes in sudden attacks and may feel sharp, shooting or electric.
For patients, this can be frightening. A person may feel certain that a tooth is the problem. Yet dental checks may not find infection, decay or a cracked tooth.
When the pain pattern does not fit
A dental problem may cause constant aching, sensitivity, swelling, pain when biting, bad taste, fever or visible changes around the tooth or gum. By contrast, trigeminal neuralgia often causes sudden bursts of severe pain that stop as abruptly as they start.
The NHS describes trigeminal neuralgia attacks as short and unpredictable, usually lasting from a few seconds to around two minutes.
Trigeminal neuralgia may be possible where pain is:
- sudden, severe and sharp
- electric-shock-like
- mostly on one side of the face
- felt in the jaw, teeth, gums or cheek
- triggered by brushing teeth, eating, speaking, washing, shaving, touch or cold air
- brief but repeated
- hard to explain after dental causes have been checked
These signs do not prove trigeminal neuralgia. However, they should prompt a medical review, especially when dental causes have been ruled out.
Why this matters
TNA UK hears from people who spent months, and sometimes years, trying to understand severe facial pain. Some first went to a dentist because the pain felt as if it came from the teeth or gums. Others had repeated appointments before anyone considered trigeminal neuralgia.
This is not about blaming dentists. Dentists play a vital role in ruling out dental causes. The issue is not blame. It is recognition.
When dental checks do not explain severe, electric-shock-like facial pain, trigeminal neuralgia should be considered. Early recognition matters because untreated or poorly controlled TN can affect eating, speaking, sleeping, working, confidence and mental health.
 For dental professionals
For dental professionals
Dentists are often the first professionals patients trust with facial pain. That places dental teams in a crucial position.
Consider trigeminal neuralgia, where pain is sudden, severe, electric-shock-like, mostly one-sided, triggered by light touch or brushing, and not explained by examination or X-ray.
Facial pain can be difficult to diagnose. In practice, dental pain and nerve pain may overlap in the way patients describe them. However, where the clinical picture does not fit dental disease, it is reasonable to consider non-dental causes, including trigeminal neuralgia.
Guidance from the Faculty of Dental Surgery at the Royal College of Surgeons of England states that TN pain is often felt in or around the mouth and may be mistaken for a toothache. It also notes that potentially avoidable dental treatment can occur because TN pain and dental pain can be similar.
Because some dental treatments are irreversible, careful assessment matters where the clinical evidence for dental disease is weak and the pain has a classic trigeminal neuralgia pattern. In those circumstances, medical assessment or referral may help prevent delay and support safer care.
When patients should speak to a GP
Patients should speak to a GP if they have frequent or persistent facial pain, especially if a dentist cannot find a dental cause. They should also seek help if the pain is severe, repeated, electric-shock-like or triggered by everyday activities.
NICE guidance says clinicians should examine the face and oral cavity, including the trigeminal nerves, to rule out dental causes and identify abnormalities that need specialist referral.
A GP may ask about the pain pattern, how long attacks last, which part of the face is affected and what triggers the pain. These details matter. Patients may find it helpful to keep a short pain diary before their appointment.
Patient checklist before an appointment
Before seeing a dentist, GP or specialist, write down:
- where the pain is
- How long do attacks last
- What the pain feels like
- What triggers it
- Whether it feels electric, stabbing, burning or aching
- Whether it affects eating, speaking or brushing teeth
- Whether dental checks found a clear cause
- Whether dental treatment helped
- Whether cold air, light touch, chewing or washing makes it worse
- What medicines or treatments have you already tried
Clear details can make an assessment easier.
What treatment may involve
Treatment depends on the diagnosis, medical history and clinical assessment.
The NHS states that carbamazepine is currently the only medicine licensed in the UK to treat trigeminal neuralgia. However, it can cause side effects and may become less effective over time for some people.
NICE CKS advises that if carbamazepine is contraindicated, ineffective or not tolerated, clinicians should seek specialist advice or refer to a neurologist or specialist pain service.
Patients should not start, stop or change medication without medical advice.
Why faster recognition matters
Faster recognition does not mean rushing to label every facial pain episode as trigeminal neuralgia. It means asking the right questions earlier.
Is the pain sudden?
Is it electric-shock-like?
Does it come in brief attacks?
Does light touch trigger it?
Does brushing teeth set it off?
Has dental disease been ruled out?
These questions can help patients avoid long delays. They can also help dentists, GPs and specialists work together.
What TNA UK believes should change
TNA UK believes trigeminal neuralgia should be recognised earlier across dental and primary care settings.
That means better awareness among dentists, GPs and frontline clinicians. It also means clearer referral routes when dental causes do not explain the pain, better patient information, proper medication review and quicker access to specialist advice where needed.
Patients should not have to prove how serious the pain is every time they ask for help.
Why this matters for dental education
Dentists do not need to diagnose every facial pain condition. However, they do need to recognise when the pattern does not fit ordinary dental disease.
A short, practical session on trigeminal neuralgia can help dental teams ask better questions, recognise red flags, avoid delay and know when medical assessment may be appropriate.
TNA UK can support dental teams with patient insight, lived experience, helpline knowledge and clear information about how TN affects everyday life.
Aneeta Prem MBE, CEO of TNA UK, is available to speak to dental professionals, universities, dental schools, conferences and training events about the patient impact of trigeminal neuralgia, delayed recognition and the importance of joined-up dental and medical care.
“The issue is not blame. It is the gap that opens when pain sounds dental but behaves like nerve pain.”
Invite TNA UK to speak
TNA UK can provide patient-led education for dental teams, universities, conferences and professional training events. To discuss a talk or training session, contact [email protected] or call 0800 999 1899.
Related TNA UK dental guidance
For further information, TNA UK has additional resources on dental pain, urgent dental care and trigeminal neuralgia:
- Trigeminal neuralgia and dental pain
- Urgent dental care and trigeminal neuralgia
- Dental guide
- Dental advice
- Trigeminal neuralgia triggers
Support from TNA UK
TNA UK supports people living with trigeminal neuralgia and facial pain through information, helpline support, e-helpline support, Regional Support Groups, webinars, conferences and patient voice.
For information and support:
TNA UK Helpline: 0800 999 1899
Email: [email protected]
Website: https://www.tna.org.uk
If someone is in immediate danger, call 999 or go to A&E. For urgent mental health support in England, call NHS 111 and choose the mental health option. Samaritans can be contacted free on 116 123 for emotional support.
FAQs
Can trigeminal neuralgia feel like a toothache?
Yes. Trigeminal neuralgia can cause pain in the jaw, teeth or gums. That is why many people see a dentist before they see a GP or specialist.
How do I know if it is a toothache or trigeminal neuralgia?
Only a qualified professional can diagnose the cause. However, trigeminal neuralgia often causes sudden, severe, electric-shock-like pain that comes in short attacks and may be triggered by brushing teeth, chewing, talking, touch or cold air.
Can brushing teeth trigger trigeminal neuralgia?
Yes. Brushing teeth, touching the face, chewing, speaking and cold air can trigger attacks in some people.
Can trigeminal neuralgia lead to avoidable dental treatment?
It can. Guidance from the Faculty of Dental Surgery states that TN pain may be mistaken for a toothache and that potentially avoidable dental treatment can occur because TN pain and dental pain can be similar.
What should I do if dental treatment does not help?
Speak to your GP and explain the pattern of pain. Include details such as attack length, triggers, location and whether dental checks found a clear cause.
Source list
- NHS. Trigeminal neuralgia: overview, symptoms and diagnosis.
- NICE CKS. Trigeminal neuralgia.
- Faculty of Dental Surgery, Royal College of Surgeons of England. Guidelines for the management of trigeminal neuralgia.
- NHS. Trigeminal neuralgia: treatment.
External links
- NHS trigeminal neuralgia overview
- NHS trigeminal neuralgia diagnosis
- NHS trigeminal neuralgia treatment
- NICE CKS trigeminal neuralgia
- Royal College of Surgeons Faculty of Dental Surgery TN guidance
Author: Aneeta Prem MBE, CEO, Trigeminal Neuralgia Association UK, 16 May 2026, London