 Swedish Trigeminal Neuralgia Study: What Patients Need to Know
Swedish Trigeminal Neuralgia Study: What Patients Need to Know
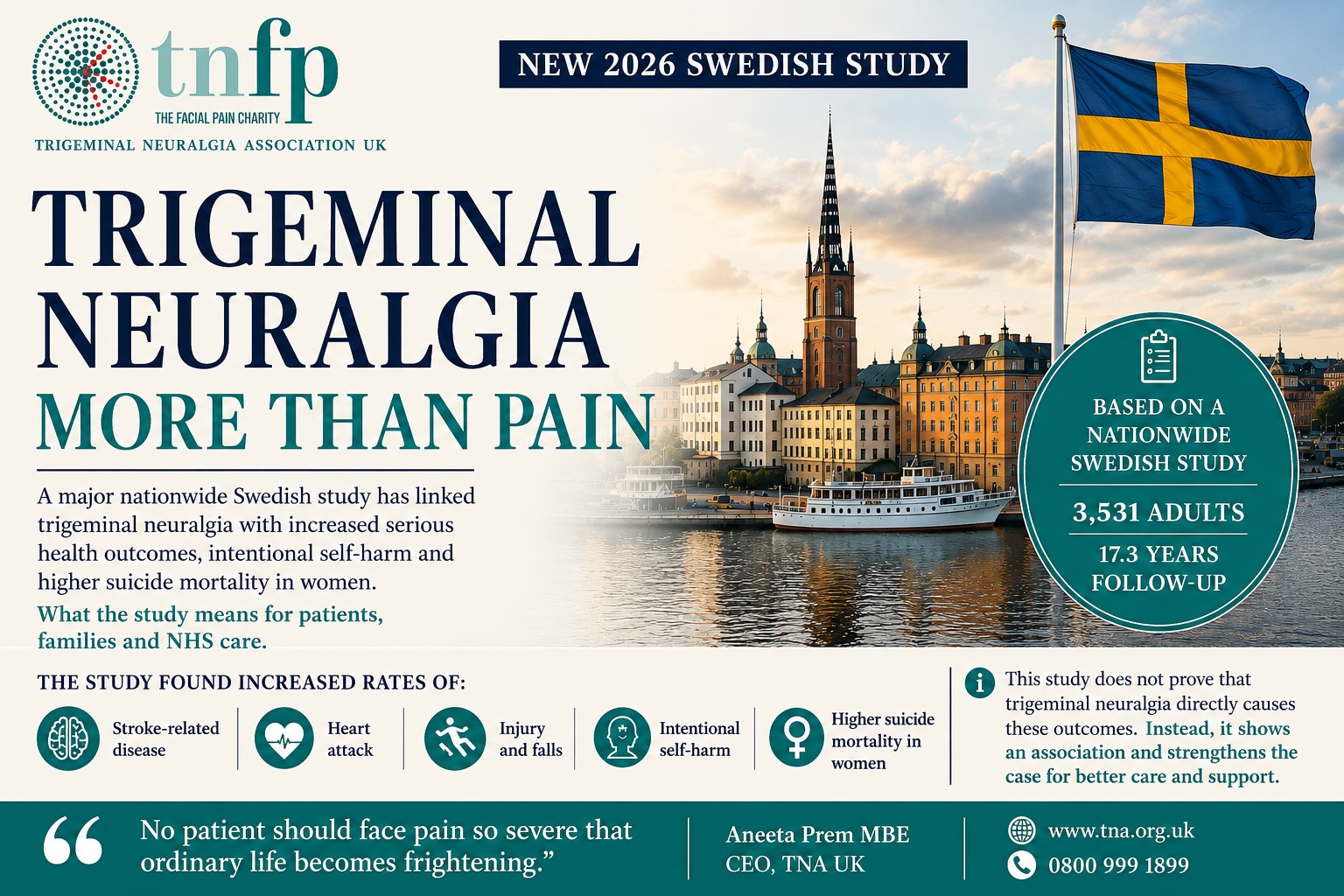
A major Swedish trigeminal neuralgia study has reported serious long-term associations between TN, physical health, injury, self-harm and patient safety. However, the findings do not prove that trigeminal neuralgia directly caused these outcomes. Instead, they show why TN must be treated as a severe neurological pain condition, not dismissed as ordinary facial pain.
study link
Why the Swedish trigeminal neuralgia study matters
Trigeminal neuralgia is not simply a pain diagnosis.
For many people, it affects safety, independence, work, family life, mental health and confidence. Because the pain can be sudden, severe and unpredictable, ordinary daily tasks may become difficult.
Eating, speaking, washing, brushing teeth, working, sleeping and going outside in cold wind can all become frightening.
NHS information describes trigeminal neuralgia as sudden, severe facial pain. It is often felt in the jaw, teeth or gums. As a result, some people first think they have a dental problem.
This Swedish trigeminal neuralgia study matters because it looked at long-term outcomes. Researchers followed adults diagnosed with trigeminal neuralgia between 2001 and 2005. Importantly, the median follow-up was more than 17 years.
What the study found
Researchers found that people with trigeminal neuralgia had higher rates of several serious outcomes when compared with the general population.
These included:
- stroke-related disease
- heart attack
- injury
- poisoning
- falls
- intentional self-harm
- higher suicide mortality among women
The study reported 14 deaths by suicide, compared with 8 expected. Among women, suicide mortality was more than doubled.
These findings are serious. However, they must be explained carefully.
Crucially, the study does not mean every person with trigeminal neuralgia is at risk. Nor does it prove that TN directly caused these deaths. Instead, it shows an association. In plain English, these outcomes appeared more often in the TN group than expected.
The key numbers
The Swedish trigeminal neuralgia study included 3,531 adults diagnosed with TN.
Of those patients, 2,326 were women and 1,205 were men. The median age at diagnosis was 65.
Researchers followed the cohort for a median of 17.3 years. Overall, this covered 50,916 patient-years.
The study found:
- intentional self-harm was increased, with a standardised incidence ratio of 2.1
- overall suicide deaths were 14 observed, compared with 8 expected
- suicide mortality among women was more than doubled, with a standardised mortality ratio of 2.5
- overall mortality was not increased
The safest summary is clear. The study found increased illness, injury and intentional self-harm in people with trigeminal neuralgia. It also found increased suicide mortality among women. However, it did not find increased overall mortality.
What this means for people living with TN
This research gives evidence to what many patients already know. Trigeminal neuralgia can affect the whole person.
It can affect:
- pain
- sleep
- eating
- speech
- confidence
- work
- family life
- mental health
- independence
- safety
For some patients, the pain is not only severe. It is also unpredictable. Because of that uncertainty, ordinary life can feel frightening.
No patient should face pain so severe that daily life becomes something to survive rather than live.
What the study does not prove
This section matters for credibility.
The Swedish trigeminal neuralgia study does not prove that TN causes suicide, stroke, heart attack or injury.
Researchers looked at health records and compared outcomes. Therefore, this type of study can show a link, but it cannot prove cause and effect.
In addition, the authors called for more research on causality and early treatment, including surgical intervention where appropriate.
That careful distinction protects patients and keeps the discussion accurate.
Why patients should not be frightened by the findings
Patients should not feel frightened by this study. Instead, they should feel believed.
The findings support what many people with TN already know. Severe facial pain can affect the whole person. It is not weakness. It is not exaggeration. It is not “just pain”.
Patients need faster recognition, clearer diagnosis, better pain control, proper medication review and access to specialist advice.
Alongside medical care, they also need emotional support, practical support and support for families and carers.
Professionals need to understand the fear that comes with unpredictable pain. A short appointment may not capture the effect of living every day with the possibility of another attack.
Why this matters for GPs and dentists
Many people with TN first feel pain in the teeth, jaw or gums. Consequently, some patients see a dentist before they see a GP or specialist.
This matters because patients can spend months or years moving between dental and medical appointments before TN is recognised.
During that time, pain may worsen. Fear may grow. Confidence may collapse.
TNA UK believes GPs, dentists and frontline clinicians need stronger awareness of trigeminal neuralgia. Earlier recognition can reduce distress and help patients reach the right care sooner.
Why this matters for NHS pathways
The NHS recognises trigeminal neuralgia as a severe facial pain condition.
NHS guidance also states that carbamazepine is currently the only medicine licensed in the UK to treat trigeminal neuralgia.
However, medication may not work for everyone. Some patients cannot tolerate side effects. Others may need specialist review, different options or further investigation.
NICE guidance on chronic pain stresses the importance of a person-centred assessment and a care and support plan. Therefore, clinicians should look at the causes and effects of pain, not only the pain score.
The Swedish trigeminal neuralgia study adds weight to the argument that TN pathways must improve.
That means:
- better training
- clearer referral routes
- quicker access to specialist advice
- proper review when medication is not working
- serious attention to mental health and safety
- better support for people living with long-term pain
A pathway that only asks whether pain exists is not enough.
Clinicians also need to ask whether the person can eat, sleep, speak, work, leave home, maintain relationships and feel safe.
Why this matters for funding
This study should matter to funders and commissioners.
If TN is linked with serious illness, injury, intentional self-harm and suicide mortality, patient support cannot be treated as optional.
Funding patient support is not a soft extra.
For people living with TN, trusted information, helpline support and peer connection can make the difference between isolation and being able to keep going.
That is why TNA UK’s Freephone helpline and e-helpline matter. Patients need more than a diagnosis. They need support to live with the condition.
TNA UK Freephone helpline: 0800 999 1899
E-helpline: [email protected]
TNA UK’s view
The Swedish trigeminal neuralgia study should mark a turning point.
Trigeminal neuralgia must be recognised as a serious neurological pain condition with physical, emotional and social consequences.
Too often, systems dismiss facial pain as a minor complaint. In practice, patients may have to explain the severity of TN again and again.
Meanwhile, many people wait too long to feel believed.
Aneeta Prem MBE, CEO of TNA UK, said:
“People living with trigeminal neuralgia have told us for years that this condition affects far more than the face. The Swedish study gives powerful evidence to the seriousness of what patients already know. The response must be faster recognition, better referral, proper support and serious investment in research. No patient should face pain so severe that ordinary life becomes frightening.”
If someone feels unsafe
If someone is in immediate danger, call 999 or go to A&E.
For urgent mental health support in England, call NHS 111.
Samaritans can be contacted free on 116 123 for emotional support.
TNA UK can listen, support, signpost, record concerns and escalate where appropriate. However, TNA UK cannot assess suicide risk, give clinical advice or manage a mental health crisis.
TNA UK Freephone helpline: 0800 999 1899
E-helpline: [email protected]
FAQs
What is the Swedish trigeminal neuralgia study?
It is a nationwide Swedish study of adults diagnosed with trigeminal neuralgia between 2001 and 2005. Researchers used national health and death registers to compare long-term outcomes with those expected in the general population.
What did the Swedish trigeminal neuralgia study find?
The study found increased rates of stroke-related disease, heart attack, injury, poisoning, falls and intentional self-harm. It also found higher suicide mortality among women with trigeminal neuralgia.
Does the study prove that trigeminal neuralgia causes suicide?
No. The study shows an association. It does not prove that trigeminal neuralgia directly causes suicide.
Does this mean every person with TN is at risk?
No. The study does not mean every person with TN is at risk. Instead, it means severe TN needs to be taken seriously, including its effect on daily life, mental health and safety.
Why is trigeminal neuralgia sometimes called the suicide disease?
The phrase has been used historically because of the extreme severity of the pain. TNA UK uses it carefully. It should never be used to frighten patients.
What should patients do if pain affects their mental health?
Patients should speak to their GP, specialist or care team. If someone is in immediate danger, they should call 999 or go to A&E. For urgent mental health support in England, call NHS 111.
What should the NHS do differently?
The NHS should improve awareness, diagnosis, referral pathways, specialist access, medication review, patient support and research into long-term outcomes.
Aneeta Prem MBE
London
15 May 2026
links to read more
Link Swedish trigeminal neuralgia study to:https://link.springer.com/article/10.1186/s10194-026-02368-1
Link NHS trigeminal neuralgia guidance to:https://www.nhs.uk/conditions/trigeminal-neuralgia/
Link NHS trigeminal neuralgia treatment guidance to:https://www.nhs.uk/conditions/trigeminal-neuralgia/treatment/
Link NICE chronic pain guidance to:https://www.nice.org.uk/guidance/ng193
Link NHS urgent mental health support to:https://www.nhs.uk/nhs-services/mental-health-services/where-to-get-urgent-help-for-mental-health/
Link Samaritans to:https://www.samaritans.org/how-we-can-help/contact-samaritan/
trigeminal neuralgia and dental pain thttps://www.tna.org.uk/news/trigeminal-neuralgia-and-dental-pain/
toothache or trigeminal neuralgia https://www.tna.org.uk/news/toothache-or-trigeminal-neuralgia/
trigeminal neuralgia and mental healthhttps://www.tna.org.uk/news/trigeminal-neuralgia-and-mental-health-2/
donate https://www.tna.org.uk/donate/