Trigeminal neuralgia in women: key insights for International Women’s Day
Trigeminal neuralgia in women can no longer be treated as a minor footnote in pain policy. Instead, the evidence shows a clear female majority and a heavy long-term burden. Therefore, International Women’s Day is a good moment to set out the facts, based on published global research and the TNA UK Patient Experience Survey.
Trigeminal neuralgia in women: the female majority in the data
Global epidemiology repeatedly reports more cases of trigeminal neuralgia in women than in men. Moreover, a large 2026 synthesis of international studies supports the same direction of travel: women appear more frequently affected across pooled datasets.
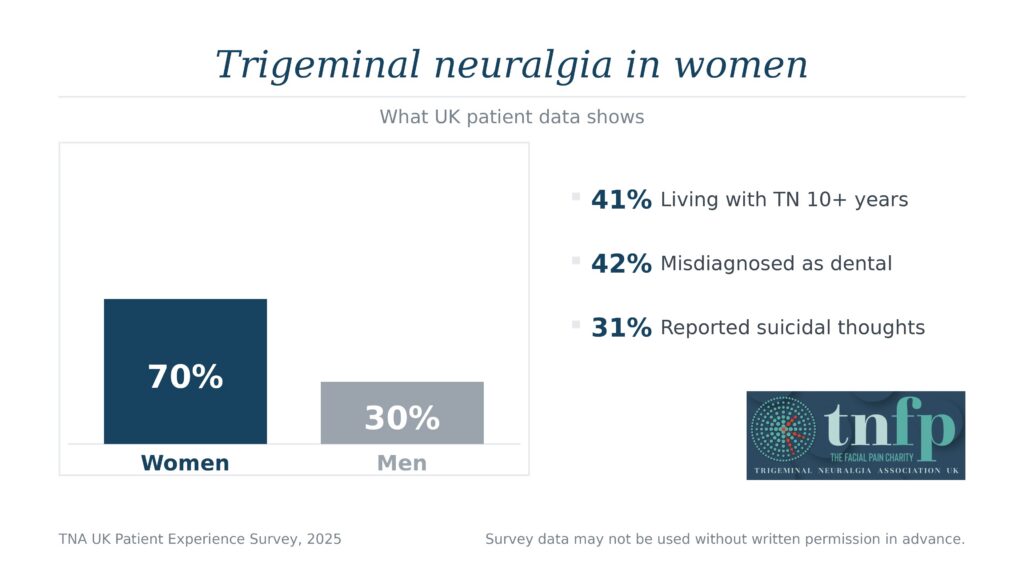
TNA UK’s own data points in the same way. In the TNA UK Patient Experience Survey (2025), respondents reported:
-
Women: 70%
-
Men: 30%
That is not a marginal skew. As a result, trigeminal neuralgia in women should sit inside serious discussions about women’s chronic pain, later-life health, and avoidable distress.
Why is trigeminal neuralgia in women a long-term condition
People often describe TN as “attacks”. However, the survey shows a long duration for a substantial proportion of respondents.
-
41% reported living with TN for more than ten years.
That single statistic matters because long duration drives cumulative harm. For example, it increases medication exposure, reduces daily function over time, and pushes many people into social withdrawal. In practice, chronic pain shrinks choices: eating, speaking, washing, and leaving home can all become risky.
Misdiagnosis and dental detours in trigeminal neuralgia in women
Misdiagnosis does not just delay treatment. It also adds procedures, fear, and exhaustion. Importantly, the survey shows a high rate of dental misdirection:
-
42% reported an initial dental misdiagnosis.
Many people described repeated dental referrals before anyone considered trigeminal neuralgia. Consequently, the system can unintentionally normalise avoidable harm. This is a practical commissioning issue, not a niche complaint.
Mental health risk signals in trigeminal neuralgia in women
The survey shows a severe psychological impact across the cohort. Meanwhile, the female majority means these risks land heavily on women living with TN.
Reported outcomes include:
-
80% reported a negative impact on mental well-being
-
31% reported suicidal thoughts
-
64% of those did not disclose suicidal thoughts to a healthcare professional
These figures require careful interpretation. They do not prove biological causation. However, they do show a serious risk signal in a predominantly female cohort. Therefore, services should not treat mental health as an optional extra or a separate referral that never happens.
If you feel at immediate risk, treat that as urgent and seek emergency help now.
Medication burden in trigeminal neuralgia in women
Medication can help. However, many people also report intolerable side effects. In the survey:
-
88% reported trying anticonvulsant medication.
When trigeminal neuralgia in women dominates the patient population, medication tolerability becomes a women’s health issue. It affects work, caring responsibilities, driving, cognition, and independence. Therefore, services should actively monitor side effects and review treatment promptly when someone cannot function.
What the evidence shows and what it does not
This page stays precise.
What the evidence shows
-
Trigeminal neuralgia in women appears to be more common in international datasets.
-
The TNA UK survey shows a strong female majority, long duration, high distress, and frequent misdiagnosis.
What the evidence does not show
-
It does not prove why women are affected more often.
-
It does not provide hormone data or menopause-linked mechanisms.
-
It does not provide sex-stratified treatment trials from the survey.
-
It does not tag survey quotes by gender.
That honesty strengthens credibility. Moreover, it keeps the argument defensible.
What should change next for trigeminal neuralgia in women
TNA UK will continue to push for practical change, as the data points to avoidable harm.
-
Earlier recognition
Clinicians should consider TN sooner, especially when dental pathways repeat without benefit. -
Joined-up pathways
Dentistry, primary care, neurology, and pain services should coordinate rather than pass patients along. -
Active mental health safeguarding
Services should ask directly about suicidal thoughts and support disclosure safely, because many people do not volunteer it. -
Realistic support for chronicity
Long-term TN needs long-term planning, not short appointments and fragmented referrals.
 Support from TNA UK
Support from TNA UK
If you are living with trigeminal neuralgia, you do not need to carry it alone. TNA UK provides information, practical support, and community connection.
Sources
-
TNA UK Patient Experience Survey (2025), internal dataset summary. TNA UK survey data may not be used, reproduced, or cited without prior written permission from TNA UK.
-
Jeong YD et al., Global incidence and prevalence of trigeminal neuralgia, 1945–2024: a systematic review and meta-regression analysis, Journal of Clinical Neurology (2026).
-
Full expert analysis by Aneeta Prem:
Aneeta Prem 28 Febuary 2026 london